The Roadmap Out of Addiction
How to escape the blur
Addiction is often treated as if one diseased part of a person must be cut out and destroyed. That framing misses something essential: for many people, the addictive part began as a protector.
As Gabor Maté has argued, the better question is often not “Why the addiction?” but “Why the pain?” Addiction is not best understood as a moral failing, but as a maladaptive attempt to survive pain. It is often an effort to numb shame, regulate overwhelm, blunt loneliness, or escape what otherwise feels unbearable. If recovery approaches that part as something to be annihilated, it will often fight back as though it is under a death sentence. Real recovery is not about pretending that part never existed. It is about building a life in which its services are no longer required.
The people who profit from the blur
Protectors can become jailers. To understand why recovery is so difficult, we have to look beyond the substance itself and into the social ecosystem surrounding it: the people, incentives, and environments that quietly benefit when a person stays sick.
Some people profit from another person’s addiction. They may not say it outright. They may not even understand it consciously. But they still benefit from lowered boundaries, impaired judgment, cheap labor, easy access, emotional chaos, or the social rewards of proximity to someone who is unraveling.
These figures fall into recognizable roles. There is the opportunist who treats a person’s impulsivity as a utility, seeking rides, labor, sex, money, or attention from someone too compromised to say no. There is the beneficiary who profits materially: the employer who keeps calling because addiction makes a worker available and exploitable, or the tenant or landlord who gains financially from chaos. And there are the companions who normalize self-destruction by praising the risks, the money, the stories, and the version of the person that is easiest to use
Together, they form a social world invested in protecting dysfunction and discrediting anyone who threatens it.
Addiction as blurred vision
Substances do not only numb pain. They blur perception. They dissolve the edges of the self.
When addiction is active, the world becomes emotionally low-resolution. A person struggling with substance use may have trouble distinguishing between someone who loves them and someone who consumes them. Healthy relationships begin to feel inconvenient, while exploitative ones can feel vivid, immediate, and rewarding.
This blur protects the system around the addiction. It allows opportunists to present themselves as allies. It allows exploitative environments to feel like belonging. It can even turn a person into an instrument against their own future, damaging the very relationships most capable of anchoring them in reality. When perception is dulled, the people consuming the person can look sharper and more convincing than the people trying to save them.
How a person knows they have a problem
A person does not only have a problem when the amount becomes dramatic. They have a problem when the substance or compulsive behavior begins to govern judgment, distort truth, and reorganize relationships around itself.
One sign is the repeated breaking of private contracts: just one drink, just one hour, just tonight, just this once—followed by the collapse of the boundary that was supposed to hold. Another is the distortion of truth. A person starts telling themselves stories that make daily life feel acceptable: that the risk is normal, the lies are harmless, the distance in the relationship is justified, the people profiting from the chaos are “just friends,” or the concern of loved ones is overreaction.
Judgment also starts to invert. Low-reward, high-risk behavior begins to feel reasonable simply because the nervous system has become organized around the next hit of relief, validation, or escape. What once would have felt reckless now feels ordinary.
Relationships are often the clearest diagnostic test. When the people who benefit from the dysfunction feel easier to be around than the people who tell the truth, something deeper than stress is happening. When honest concern feels like persecution, when a partner starts to feel like an inconvenience, when defensiveness rises immediately to protect the system, the problem is no longer just use. It is governance.
Sometimes the simplest test is the smallest one: Can I stop just for today? If the thought of twenty-four hours without the substance, the behavior, or the social world built around it triggers panic, bargaining, rage, or dread, that is not nothing. It is information.
If you are asking whether you have a problem, that question itself may be a flare rising through the fog.
Addiction as a counterfeit community
Addiction can also function like a kind of cult. It creates its own language, loyalties, permissions, and punishments. It rewards secrecy, disappearance, broken boundaries, and betrayal of the very people trying to keep someone alive.
In that ecosystem, the healthy influence is often recast as controlling, joyless, or oppressive, while the people feeding the dysfunction are treated as freedom, loyalty, and belonging. The person is rewarded for every lie told, every boundary crossed, every relationship neglected, every night vanished into the blur. Little by little, the system encourages them to push away the people and structures most likely to help them survive.
Threats to the status quo are rarely confronted honestly. They are tried, mocked, and slowly erased. The people who challenge the blur are recast as unstable or toxic, while the people feeding the dysfunction are treated as insiders. A kind of mob logic takes over. The group reinforces every lie, every disappearance, every reckless choice, and every betrayal that helps sever the person from reality. They do not need to attack the healthy influence directly. They only need to make the person carry out the exile for them.
That reversal is one of the clearest signs that the system has taken hold: not only is the substance protected, but everyone who threatens it is slowly marked for removal.
Recovery requires new eyes
Because addiction distorts judgment, recovery cannot rely on solitary insight alone. In the early stages, people often need to borrow the eyes of others.
A real recovery team consists of people with no secondary gain in the person’s suffering, and different helpers do different jobs. Therapists and addiction counselors help identify patterns, triggers, trauma, and the underlying logic of the compulsive system. Physicians and other medical providers help with detox, medication, and safety. Sponsors and recovery groups provide structure, accountability, and a counter-community to the social world organized around use.
Peer support specialists deserve special mention. People with lived experience in recovery often see dangers that others can miss. They may recognize bargaining, disappearance, manipulation, false confidence, and social pressure not because they studied them in theory, but because they survived them. That does not make clinical care less important. It makes peer support a different kind of intelligence, one grounded in recognition.
In the United States, that team might include licensed therapists, addiction counselors, physicians, sponsors, and certified peer support specialists. In Canada, the titles vary by province, but the same functions may be carried by registered psychotherapists, social workers, addiction counsellors, physicians, sponsors, peer recovery workers, or lived-experience supporters. The names differ. The need does not.
Whatever the titles, the goal is the same: to interrupt the lie. These helpers help a person distinguish remorse from self-destruction, loneliness from love, and a setback from a death wish.
Recovery happens in stages
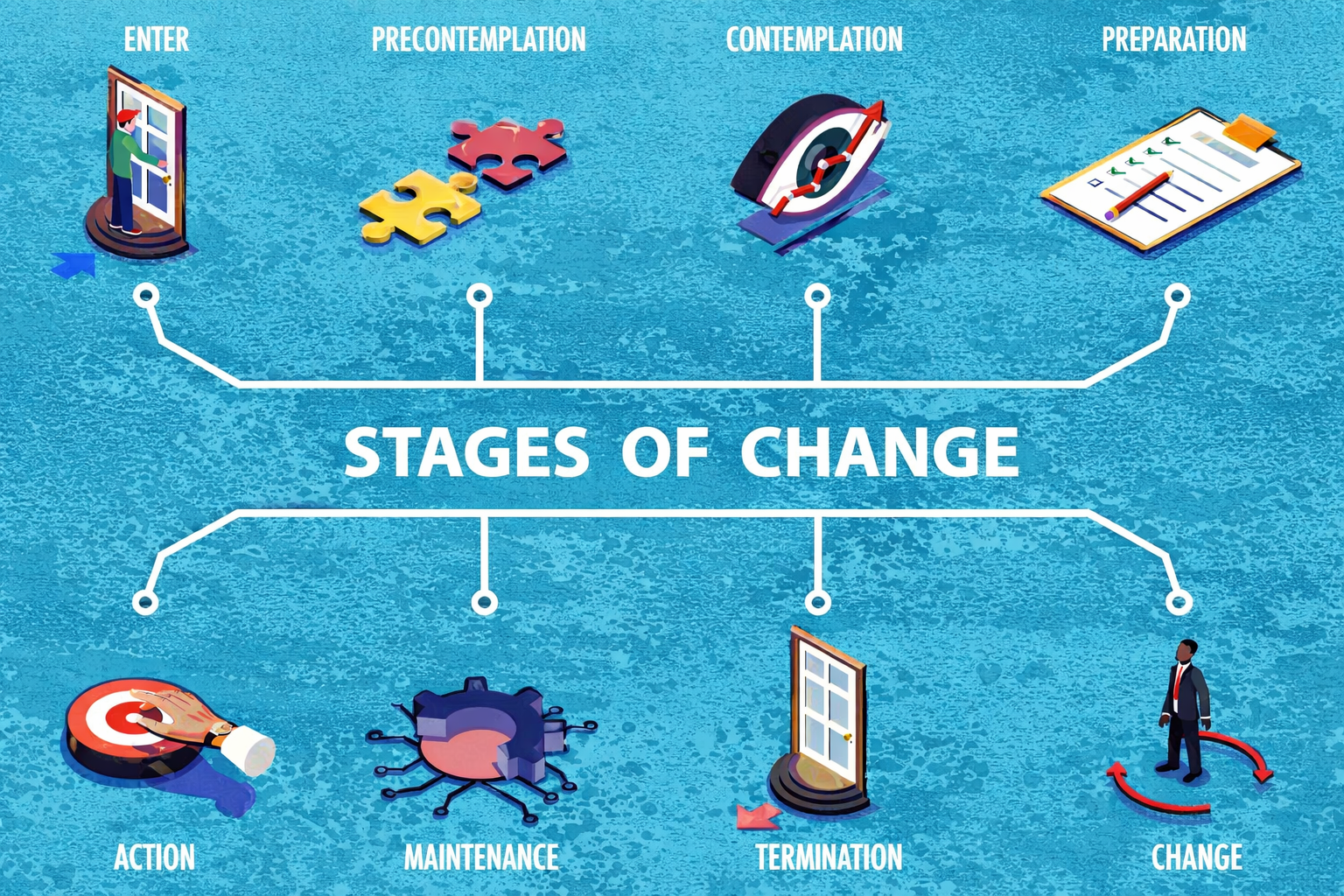
Recovery is rarely a single decision. More often, it unfolds in stages.
A person may begin in pre-contemplation, where the addiction still feels necessary and the cost of change seems greater than the cost of staying the same. Then comes contemplation, the stage of ambivalence, where one part of the person can see the damage while another still believes the substance is helping them survive.
Preparation begins when insight turns into practical movement: researching treatment, going to a meeting, telling the truth to one person, considering a different environment. Action is the visible stage, when behavior starts to change and the old coping system begins to loosen its grip. Maintenance is not just staying abstinent, but learning how to live differently enough that the addiction no longer feels like the only available relief.
This process is rarely linear. People often move through these stages more than once. That does not mean change is fake or impossible. It means recovery is usually a spiral, not a straight line.
Recovery also requires structure
Insight alone is rarely enough. Different forms of support serve different functions. Residential treatment can be necessary when the environment is too saturated with danger, access, instability, or medical risk for a person to interrupt the cycle on their own. Peer-based recovery groups, including 12-step programs and other mutual-aid models, offer repetition, accountability, and the steadying force of people who make sobriety feel imaginable over the long haul.
Groups also offer a safer kind of recognition. A person can hear their own life echoed in someone else’s story before they are ready to fully tell the truth about their own. That indirect recognition can lower shame and reduce defensiveness. It allows someone to learn without immediately feeling exposed.
Groups can also regulate in ways that are easy to underestimate. A person whose nervous system is stuck in chaos, vigilance, or collapse may not be able to generate calm alone. But human beings regulate each other. In the presence of people who are grounded, honest, and not escalating, distress can begin to settle. Sometimes what a struggling person borrows first is not wisdom, but steadiness. The best group is often not the most impressive one, but the one in which a person’s nervous system feels safe enough to stop lying.
This is part of why 12-step recovery has remained so durable for so many people. At its best, it offers more than meetings or slogans. It offers a structure for surrender, self-examination, confession, amends, daily inventory, and service. Whether or not a person uses explicitly spiritual language, the movement is recognizable: from denial to honesty, from isolation to accountability, from self-will to relationship, and from private chaos to a livable practice.
Some forms of withdrawal are not simply miserable. They can be dangerous. Alcohol, benzodiazepines, and barbiturates are in a different category because abrupt withdrawal can become medically serious and, in some cases, life-threatening. In those cases, detox is not a test of character. It is a medical event. For people with intense medical anxiety, supervised detox is not punishment, but safe containment.
Not all treatment is good treatment. Desperation makes people vulnerable to glossy promises, one-size-fits-all programs, and facilities more interested in billing than healing. Recovery is not made durable by a dramatic thirty-day interruption alone, but by what follows it.
Predatory treatment deserves special caution. Some programs market themselves as salvation while functioning more like intake funnels, billing machines, or soft-focus holding tanks. Grand promises, vague staffing, pressure to commit immediately, and polished sales language without clear clinical answers are all warning signs. A legitimate program should be transparent about who provides care, whether medical detox is available when needed, how co-occurring mental health issues are treated, what the daily schedule includes, and what happens after discharge. Bad treatment is dangerous not only because it wastes money or time, but because it can convince a person that “nothing works” when what failed was the quality of care.
Another emerging area of treatment is psychedelic-assisted therapy, particularly with psilocybin and, more controversially, ibogaine. The promise here is real enough to take seriously, especially in structured clinical settings, but it should not be romanticized. These interventions are not magical cures; they are openings. What matters is not only the experience itself, but the preparation, containment, and integration that follow. Without that structure, a powerful experience can become just another dramatic interruption rather than lasting change.
Recovery plans also need to account for triggers, not just ideals. Hunger, anger, loneliness, and exhaustion remain useful warning lights, but they are not the whole map. Significant dates, anniversaries, grief, celebrations, sensory cues, old routes, certain neighborhoods, particular songs, and specific people can all pull the nervous system back toward familiar escape. A real recovery plan should be written down and concrete: who to call, what to do in the first fifteen minutes of a craving, which people and places are off-limits, what daily routines reduce vulnerability, and what truths need to be read again when the mind starts bargaining.
There are also more medical options than many people realize. For opioid use disorder, medications such as buprenorphine, methadone, and naltrexone can reduce craving, withdrawal, and the reward loop that keeps a person trapped. For alcohol use disorder, medications such as naltrexone, acamprosate, and disulfiram may also play an important role. These are not signs of weakness or failed recovery. For many people, they are part of what makes recovery structurally possible.
Addiction is also broader than the substances most readily recognized. It can attach itself to screens, pornography, gambling, work, food, exercise, romance, caretaking, information, or worry—any pattern repeatedly used to regulate an overwhelmed nervous system or avoid contact with pain. The question is often not the activity itself, but the function it is serving.
Loved ones, limits, and repair
Support from loved ones matters, but so do the limits of that support. One of the most painful distinctions in addiction is the difference between helping and enabling. Helping makes recovery more possible. Enabling makes addiction easier to continue. Driving someone to treatment, telling the truth, refusing to fund chaos, and holding clear boundaries can all be acts of love. So can refusing to lie, cover, rescue, or absorb consequences that belong to the addiction.
The same principle applies to families. Groups for loved ones can help break secrecy, reduce panic, and teach the difference between support and rescue. Families often need parallel recovery of their own, because one person may be healing while the people around them are still living in the aftershocks.
Active addiction is also often highly manipulative, not necessarily because the person is monstrous, but because the addiction learns to protect its supply at all costs. It can distort reality, weaponize guilt, make promises it does not intend to keep, and recruit the hope of other people into the service of staying unchanged. This is why consequences matter. They are not the opposite of love; they are often the first form of reality strong enough to interrupt the cycle.
There is another painful limit that recovery forces into view: no one can walk through the door on another person’s behalf, and loved ones cannot afford to work harder at recovery than the person who is supposed to be living it. They can close off the exits that make self-destruction easier. They can stop funding chaos, stop lying, stop rescuing, and keep the path to treatment visible. But they cannot supply the will that recovery requires. They cannot become another adult’s executive function without being pulled into the illness themselves.
A person who gets sober only for a spouse, a parent, or a court date is often borrowing motivation from outside themselves, and borrowed motivation rarely holds when the pressure changes. At some point, the desire to live differently has to become internal. This is one of the hardest truths for families: you can make recovery more possible, but you cannot make another person choose it, and you cannot want it more than they do without losing yourself in the process.
Loved ones often deserve amends, but early recovery is rarely the moment to demand them. In the beginning, shame is still volatile, and pressure for apology can trigger collapse rather than accountability. That does not mean the harm does not matter. It means timing matters. Early recovery may require a person to focus first on stopping the damage, stabilizing, and telling the truth consistently enough that later amends can be real rather than performative. Sometimes the first amend is behavioral: staying sober today, causing no new harm, and becoming someone capable of repair.
Recovery also depends on distinguishing emotions that often get confused. Regret says, “I hate what this cost me.” Remorse says, “I hate what I did to you.” Guilt says, “I did something wrong.” Shame says, “I am something wrong.” Guilt and remorse can support repair because they leave room for action, accountability, and amends. Shame is more dangerous because it attacks identity rather than behavior. It does not ask a person to change; it tells them they are beyond change.
Self-forgiveness matters too, for both the person in recovery and the loved ones around them. But real self-forgiveness follows action; it does not replace it. It is not pretending the harm did not happen. It is refusing to let shame become the permanent ruler of the future.
Surrender, substitution, and the long middle
Recovery asks for a paradox that many people resist at first: surrender. In this context, surrender is not collapse or passivity. It is the decision to stop fighting reality with the same tools that have already failed. It is the shift from white-knuckling, bargaining, and self-deception to honesty, help, and structure. What feels like weakness at first can become a form of strength, because the person no longer has to defend the illusion that they can keep controlling what is already controlling them.
Recovery also has quieter traps. One is substitution: when the substance recedes but the same compulsive system simply migrates into work, exercise, caretaking, recovery performance, or some other socially acceptable excess. Another is boredom, flatness, or emotional deadness. After chaos, ordinary life can feel intolerably gray. That does not always mean recovery is failing; it may mean the nervous system is still learning how to live without extremes. This is why abstinence and recovery are not identical. A person can stop using without yet feeling whole.
Recovery also has recognizable arcs that can mislead people if they are not expected. Early relief can create overconfidence. Later, irritability, flatness, sleep disruption, or emotional rawness can feel like failure when they are often part of healing. Some people encounter a period of disorientation once the old coping system has loosened and a new identity has not yet fully formed. These phases are not excuses for harm, but they are important explanations.
There is also reason for hope: recovery often feels most fragile in the beginning and more stable as time, repetition, honesty, and support accumulate. The early period is often the least stable. For many people, recovery begins to stick not through one breakthrough, but through accumulated structure, repeated truth-telling, and enough time for a different life to become familiar.
It also helps to distinguish a lapse from a full collapse. A misstep should never be treated lightly, but neither should it automatically be treated as proof that recovery has failed. The useful question is not only Did the person use again? but What failed around the use? What trigger was missed? What support was absent? What structure was too weak? What truth was avoided? Recovery becomes more durable when setbacks are neither normalized into excuses nor weaponized into shame.
Why “just for today” works
To a brain shaped by trauma and dysregulated by substances, forever can feel like suffocation. This is why “Just for today, stay sober” matters. It shrinks the mountain to a manageable step.
Recovery is often won through small acts of interrupted momentum: Today I do not go where I disappear. Today I tell the truth. Today I deal with the next thing, not the whole thing.
This narrowing of focus matters because overwhelm is one of addiction’s favorite weapons. When people try to solve the next five years all at once, the nervous system often freezes. Recovery becomes more possible when the task is reduced to the step directly in front of them: the next phone call, the next meeting, the next honest sentence, the next hour without disappearing. The same is true of anxiety. It is often easier to take one fear at a time than to battle an entire future in a single sitting.
And sometimes even “just for today” is too large. In the hardest moments, recovery may need to shrink further: just for this hour, just for this conversation, just until this light turns green. The point is not denial, but scale. Before a lapse, it helps to remember that relapse is not a harmless option; for some people it is a potentially fatal threat. After a lapse, the question changes. It becomes: What failed, and what has to change so I do not die from the same mistake next time?
The social break
The hardest part of recovery is often not simply giving up the substance. It is surviving the consequences of clarity. When a person begins to heal, the ecosystem often pushes back. The people who benefited from confusion may mock the change, question the boundaries, or call the sober person boring, dramatic, controlled, or “not themselves anymore.”
But of course they are not themselves anymore. That is the point.
Recovery threatens every arrangement that depended on blur. Sometimes sobriety means discovering that what looked like friendship was access, what looked like freedom was usefulness, and what looked like acceptance was simply tolerance for self-destruction. To recover, a person often has to become willing to be cast out of the social world that fed on their confusion.
What returns
What makes recovery worth it is not only the absence of the substance, but the return of ordinary life in high resolution. Sleep becomes real again. Memory becomes less fragmented. A person can wake up without dread, speak without performing, and come home without carrying a second life in their body. Trust rebuilds slowly, then unexpectedly. Food tastes better. Mornings stop feeling like punishment. The nervous system learns that peace is not emptiness.
And some rewards cannot be premeditated. They do not arrive because a person fully understood them in advance. They arrive because, as they walk the path, the path appears. A life worth staying for is often not visible at the beginning. It emerges through repetition, honesty, and the slow return of reality. What first feels like deprivation begins, over time, to feel like relief: fewer shadows, fewer lies, fewer people feeding on the blur. What remains is smaller, quieter, and infinitely more real.
The next 24 hours
If recovery begins anywhere, it begins here:
Identify the stakeholders: Who loses access, money, status, or convenience if I stay sober today?
Check the basics: Am I hungry, angry, lonely, or tired?
Call someone who has nothing to gain from my confusion.
Sign the smallest contract that still matters:
Just for today, I will stay sober.
Just for today, I will not go where I disappear.
Just for today, I will let reality be real.
Resources: United States, Canada, dual diagnosis, international, and 12-step groups
United States
988 Suicide & Crisis Lifeline for immediate crisis support, available 24/7 by call or text.
SAMHSA Find Help for behavioral health support and treatment resources related to mental health, drugs, and alcohol.
FindTreatment.gov to search U.S. treatment facilities for substance use and mental health disorders, including opioid treatment options.
Canada
Canada.ca: Get help with substance use for national, provincial, and territorial substance use supports, including overdose prevention and referral information.
Canada.ca: Mental health support / Get help for crisis, mental health, and substance use support, including 9-8-8 information and provincial or territorial pathways.
Dual diagnosis / co-occurring mental health and substance use
In the U.S., FindTreatment.gov includes both mental health and substance use facilities in one locator.
In Canada, the term concurrent disorders is commonly used for co-occurring addiction and mental health problems; national and provincial pathways typically route through broader mental health and substance use services.
International / multiple countries
Find a Helpline (LifeLine International) is a global directory of helplines by country and topic, including substance use and mental health support in many regions.
World Health Organization mental health and substance use program for global guidance and country-system context.
12-step groups
Alcoholics Anonymous (AA) meeting finder and local contacts for in-person and online meetings in the U.S., Canada, and internationally.
Narcotics Anonymous (NA) meeting search for local NA communities and virtual meetings.
Al-Anon / Alateen for families, partners, and teenagers affected by someone else’s drinking, with in-person, phone, online, and worldwide meeting options.
Adult Children of Alcoholics & Dysfunctional Families (ACA/ACoA) meeting finder for in-person, online, and phone meetings.
If withdrawal could be dangerous
If a person has been using alcohol, benzodiazepines, or barbiturates regularly, do not treat stopping as a solo willpower test. Seek medical advice or urgent care support because withdrawal can be medically dangerous.
If there is immediate danger, call 911. In the U.S., call or text 988. In Canada, call or text 9-8-8 or use local emergency services.